The Problem
A patient comes to the doctor concerned about longstanding fatigue symptoms. She knows of a family history of underactive thyroid disease and is worried her thyroid is not working properly
Introduction and some basic concepts
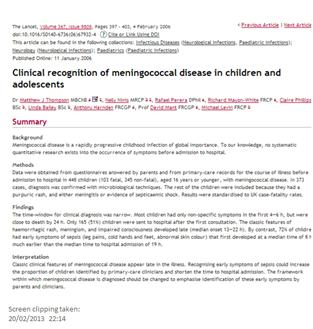
[from Basic endocrinology : for students of pharmacy and allied health sciences, edited by Constanti et al (1998; ISBN 9780203301739) ]
The thyroid gland lies in front of the trachea below the larynx. The hypothalamus and pituitary control normal secretion of thyroid hormones. The thyroid hormones in turn control the body’s metabolism. The two active hormones are iodinated derivatives of the amino acid tyrosine. Nearly 90% of the output is thyroxine (T4) containing four iodine atoms while nearly 10% of the output is triiodothyronine (T3) containing three iodine atoms. In health < 1% “reverse” T3 (rT3) is released; this increases in presence of severe illness or starvation. In the bloodstream the thyroid hormones are extensively bound to plasma proteins, principally thyroxine binding globulin (TBG).
Note that in patients on T4 replacement all T3 is produced by peripheral conversion, and so circulating T4 levels may need to be maintained slightly above the “normal” reference range to generate adequate tissue T3 concentrations.
So far so good that is what medical students and other healthcare professionals have been taught to decades. The thyroid stimulating hormone from the pituitary goes up when/if thyroid hormone levels too low, and vice versa.
However this is not the whole story. A more detailed appreciation of the nuances of thyroid hormone metabolism are required to appreciate why so many people with underactive thyroid disease continue to struggle to regain normal health. For example, the story of Coralie Phillips and Donna Roach gives pause for thought about one of the most neglected conditions in general medicine http://www.thyroidbooks.co.uk/ .
Underactive thyroid disease (UAT) is considered simple to diagnose and simple to treat. Luckily this is the case most of the time. Unfortunately when the approach does not seem to be working effectively patients are labelled as difficult or dismissed as mentally ill instead. The medical establishment generally has failed to treat people with UAT scientifically by looking at factors which may conspire to prevent the neat outcome which is expected.
The purpose of this brief essay is to highlight these pitfalls in the hope that fewer people with UAT will suffer in future.
Modern thyroid hormone biochemistry
Role of vitamin D
It seems that adequate levels of vitamin D are necessary to maintain thyroid health.
For example (http://www.endocrine-abstracts.org/ea/0032/ea0032p1008.htm): In this study of 100 patients with autoimmune hypothyroidism compared to 100 subjects as control group, the higher vitamin D deficiency rates besides lower vitamin D levels in the Hashimoto group together with the inverse correlation between vitamin D and anti-TPO suggest that vitamin D deficiency may have a role in the autoimmune process in Hashimoto’s thyroiditis.
Conversely, some evidence emerging that high levels of T3 may suppress vitamin D levels (e.g. http://endo.endojournals.org/content/154/2/609.short) This may be one mechanism for bone losing state of untreated hyperthyroidism (or over-treatment of UAT)
Role of vitamin B12
A new abstract summarises the impact of low vitamin B12 on thyroid disease (and other [geriatric] conditions http://www.bioline.org.br/abstract?rc13008):
Vitamin B12 deficiency is a common condition in the elderly. It is repeatedly overlooked due to multiple clinical manifestations that can affect the blood, neurological, gastrointestinal, and cardiovascular systems, skin and mucous membranes. The various presentations of vitamin B12 deficiency are related to the development of geriatric syndromes like frailty, falls, cognitive impairment, and geriatric nutritional syndromes like protein-energy malnutrition and failure to thrive, in addition to enhancing aging anorexia and cachexia. Therefore, interventions must be developed to include their screening and diagnosis to make early and appropriate treatment to prevent its complications before they become irreversible.
Role of trace minerals
A detailed overview of heavy metals by a nanotechnology team illustrates how important optimising the levels can be for cellular health and ascorbic acid/Krebs cycle [http://www.ijsrp.org/research-paper-0413/ijsrp-p16110.pdf]
Iron (Fe) Contained in hemoglobin and myoglobin which are required for oxygen transport in the body. Part of the cytochrome p450 family of enzymes. Anemia is the primary consequence of iron deficiency. Excess iron levels can enlarge the liver, may provoke diabetes and cardiac falurer. The genetic disease hemochromatosis results from excess iron absorption. Similar symptoms can be produced through excessive transfusions required for the treatment of other diseases.
Copper (Cu) Contained in enzymes of the ferroxidase (ceruloplasmin?) system which regulates iron transport and facilitates release from storage. A structural element in the enzymes tyrosinase, cytochrome c oxidase, ascorbic acid oxidase, amine oxidases, and the antioxidant enzyme copper zinc superoxide dismutase. A copper deficiency can result in anemia from reduced ferroxidase function. Excess copper levels cause liver malfunction and are associated with genetic disorder Wilson’s Disease
Manganese (Mn) Major component of the mitochondrial antioxidant enzyme manganese superoxide dismutase. A manganese deficiency can lead to improper bone formation and reproductive disorders. An excess of manganese can lead to poor iron absorption.
Iodine (I) Required for production of thyroxine which plays an important role in metabolic rate. Deficient or excessive iodine intake can cause goiter (an enlarged thyroid gland).
Zinc (Zn) Important for reproductive function due to its use in FSH (follicle stimulating hormone) and LH (leutinizing hormone). Required for DNA binding of zinc finger proteins which regulate a variety of activities. A component of the enzymes alcohol dehydrogenase, lactic dehydrogenase carbonic anhydrase, ribonuclease, DNA Polymerase and the antioxidant copper zinc superoxide dismutase. An excess of zinc may cause anemia or reduced bone formation.
Selenium (Se) Contained in the antioxidant enzyme glutathione peroxidase and heme oxidase. Deficiency results in oxidative membrane damage with different effects in different species. Human deficiency causes cardiomyopathy (heart damage) and is known as Keshan’s disease.
Fluorine (Fl) Constituent of bones and teeth. Important for tooth development and prevention of dental caries. Derives from water, tea, and fish.
Cobolt (Co) Contained in vitamin B12. An excess may cause cardiac failure.
Molybdenum (Mo) Contained in the enzyme xanthine oxidase. Required for the excretion of nitrogen in uric acid in birds. An excess can cause diarrhea and growth reduction.
Chromium (Cr) A cofactor in the regulation of sugar levels. Chromium deficiency may cause hyperglycemia (elevated blood sugar) and glucosuria (glucose in the urine).
A recent Turkish paper indicates low zinc levels in saliva (and so plasma) in people with UAT [http://www.turkjem.org/sayilar/79/buyuk/1-4.pdf]. It is not known if this is a cause or effect of UAT but suggests that people with UAT should ensure zinc levels are optimised.
Role of reverse T3?
A recent study highlights the dangers of subclinical hyperthyroidism considering healthy aging associated with decline in T3, unchanged levels of T4, with rise in TSH and rT3 [http://goo.gl/WCUk8]
The process of normal aging affects the hypothalamic-pituitary-thyroid axis in a number of ways, resetting of the set point being the most important of them. Contrary to the earlier belief, longevity has been reported to be associated with high serum TSH. Most recent studies have demonstrated an age dependent decline in serum free T3 levels, whereas FT4 levels remains relatively unchanged and TSH & rT3 levels increase with age. Two recent meta-analyses have shown increased risk of adverse cardiovascular outcomes in patients younger than 65 years of age, but not in those more than 65 year old. There is a good number of evidence documenting increased mortality in elderly individual with sub- clinical hyperthyroidism, which should be kept in mind while treating mildly elevated TSH in these patients. It is also important to remember that thyroid functions in the elderly closely mimics that found in sick euthyroid syndrome.
People with UAT recognise that rT3 levels can rise while they are ill. They make a good argument that rT3 levels ought to be checked in cases of poor response to standard treatment. If rT3 is raised then clearly the the patient is ill and efforts need to be made to restore her/him to biochemical euthyroid state.
Thyroid stimulating hormone response is not predictable
A recent paper by JEM Midgley highlights the problem with depending on TSH to determine whether or not a person with thyroid disease is adequately treated [http://jcp.bmj.com/content/66/4/335.abstract and http://www.hindawi.com/journals/jtr/2012/438037/]
Our data suggest that the states of hypothyroidism, euthyroidism and hyperthyroidism can be regarded as differently regulated entities. The apparent complexity could be replicated by mathematical modelling suggesting a hierarchical type of feedback regulation involving patterns of operative mechanisms unique to each condition. For clinical purposes and assay evaluation, neither the standard model relating logTSH with FT4, nor an alternative model based on non-competitive inhibition can be reliably represented by a single correlation comparing all samples for both hormones in one all-inclusive group.
Conclusion and approach to the patient
UAT is a common condition though there is still a lot to learn how to accurately diagnose it in all patients. Even if the diagnosis is not elusive the patient’s response to treatment is occasionally not what is expected.
To ensure improved diagnostic accuracy free T3 ought to be checked for all patient suspected of suffering UAT.
Thus it is my practice to check the following in a person who presents with a longstanding history of fatigue with no obvious abnormality on physical examination:
- Full blood count with vitamin B12, folic acid and transferrin saturation index for iron status
- Thyroid function test, including free T3 as well as free T4 and TSH
- C-reactive protein
- Vitamin D level and calcium profile
If patient is proved to have UAT, treatment is started at 25 mcg daily of thyroxine. The patient will be reviewed approximately 2 months later when thyroid function is rechecked with fT3, as well as checking thyroid peroxidase autoantibody (for autoimmune thyroid disease). If there has been a poor response to treatment, copper, zinc and 9am cortisol level should also be checked. rT3 should be checked in all poor responders to treatment too; this is recommended by Thyroid UK.
For details about signs and symptoms of UAT see for example: patient.co.uk
http://www.hormone.org/diseases-and-conditions/thyroid

Some patient resources
UK
Thyroid UK – http://thyroiduk.healthunlocked.com/ http://www.thyroiduk.org.uk/tuk/index.html
International
American Thyroid Association – http://www.thyroid.org/
Association Française des Malades de la Thyroïde – http://www.asso-malades-thyroide.org/
Petition – Better Endocrinological Service and Treatment for Thyroid Patients in United Kingdom
If you agree that more should be done for people with thyroid disease, then please sign the petition here